Preoperative Geriatric Assessment - #64
Take QuizEstablish capacity for consent and the patient’s understanding of the need of surgery.
Hospital or clinic visit of an older adult considering surgical intervention
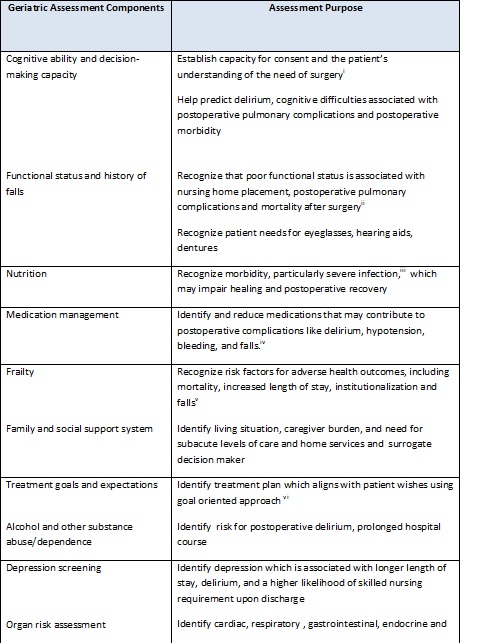
Identify key assessment areas and available tools to assist in determining appropriateness of surgical intervention in geriatric patients. This ideally includes a comprehensive interdisciplinary assessment of function, cognition, nutrition, medication management, social support, frailty. This information is then integrated with patient and family goals and preferences to develop an integrated plan for treatment and follow up.
An increasing proportion of the aging population is undergoing surgery.[i] Individuals age in different ways. Identification of frail older adults, particularly those with decreased cognitive and functional reserve, is a key component of preoperative assessment.[ii]
The increased risks of postsurgical complications in frail older adults require an individualized care process[iii] as postoperative complications increase the risk of 30-day readmission four fold, and the potential costs are high.[iv]
[i] Etzioni DA, Liu JH, Maggard MA, Ko CY. The aging population and its impact on the surgery workforce. Annals of Surgery 2003;238:170-7
[ii] Zenilman M. Geriatric surgery past, present and future .JAMA Surg 2012;147(1):10
[iii] Arora VM, Johnson M, Olson Jet al. Using acute care of vulnerable elderly quality indicators to measure the quality of hospital care for vulnerable elders. J Am Geriatr Soc 2007;55:1705-11
[iv] Sieber FE, Barnett SR. Preventing postoperative complications in the elderly. Anesthesiology Clin, 2011;29:83-97
Science Principles
-
Describe components of a preoperative geriatric assessment
-
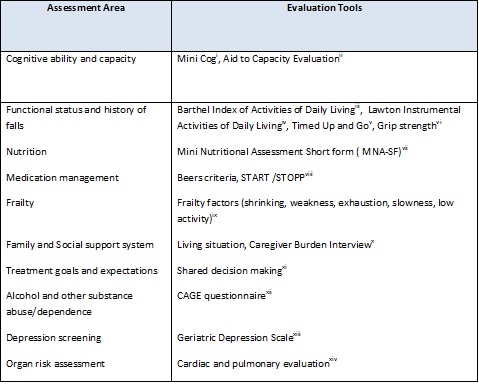
Identify available tools to assistwith preoperative geriatric assessment
Review of Systems (ROS)
Geriatric Topics
Science Principles
[i] Etzioni DA, Liu JH, Maggard MA, Ko CY. The aging population and its impact on the surgery workforce. Annals of Surgery 2003;238:170-7
[ii] Zenilman M. Geriatric surgery past, present and future .JAMA Surg 2012;147(1):10
[iii] Arora VM, Johnson M, Olson Jet al. Using acute care of vulnerable elderly quality indicators to measure the quality of hospital care for vulnerable elders. J Am Geriatr Soc 2007;55:1705-11
[iv] Sieber FE, Barnett SR. Preventing postoperative complications in the elderly. Anesthesiology Clin, 2011;29:83-97
[v] Billick SB, Perez DR, Garakani A. A clinical study of competency to consent to hospitalizations and treatment in geriatric patients. J Forensic Sci.2009;54(4):943-46
[vi] Kim S, Brooks AK, Groban L. Preoperative assessment of the older surgical patient: honing in on geriatric syndromes. Clin Interv in Aging 2015;10:19-20
[vii] Kuzu MA, Terzioglu H, gene V et al. Preoperative nutritional risk assessment in predicting postoperative outcomes in patients undergoing major surgery. World J Surg.2006:30(3);378-390
[viii] Finlayson E Maselli, Steinman MA, Rothberg MB, Lindenauer PK, Auerbach AD. Inappropriate medication use in older adults undergoing surgery: a national study. J Am Geriat Soc 2011;59(1):2139-44
[ix] Boyd CM, Xue Q-L, Simpson CF, Guralnik JM, Fried LP. Frailty, hospitalization, and progression of disability in a cohort of disabled older women. Am J Med. 2005;118(11):1225-1231
[x] Reuben DB. Medical care for the final years of life. “when you are 83,it’s not going to be 20 years”.JAMA.2009;302(24):2686-94
[xi] Dewan SK, Zheng SB, Xia SJ. Preoperative geriatric assessment: comprehensive, multidisciplinary and proactive. Euro J of Int Med 2012;23.487-490
[xii] Borson S, Scanlan M, Chen P, et al. The mini cog as a screen for dementia; validation in a population based sample. J Am Geriat Soc 2008;51:1451-54
[xiii] Etchells E, Darzins P, Silberfeld M, Molloy W, Strang D et al. Assessment of Patient Capacity to Consent to Treatment. J Gen Intern Med. 1999 Jan; 14(1): 27–34.
[xiv] Collin C, Wade DT, Davies S, Horne V. The Barthel ADL Index: a reliability study. Int Disabil Stud. 1988;10(2):61-63.
[xv] Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 1969;9(3):179-86
[xvi] Kristensen MT, Foss NB, Kehlet H. Timed "Up and Go" Test as a predictor of falls within 6 months after hip fracture surgery. Phys Ther. 2007.87(1):24-30
[xvii] Gale CG, Martyn CN, Cooper C , Sayer AA. Grip strength, body composition,and mortality. Int. J. Epidemiol. Advance Access published October 19, 2006
[xviii] Che-Sheng Chu, Chih-Kuang Liang, Chin-Liang Chu et al. Short -Form Mini nutritional assessment as a useful method of predicting the development of postoperative delirium in elderly patients undergoing orthopedic surgery. Gen Hospital Psych.2016;38:15-20
[xix] Appropriate Prescribing- Geriatrics Evaluation and Management Tools .From the American Geriatrics Society. Accessed online Feb 17th 2016
[xx] Makery MA, Segev DL, Pronovost PI, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg 2010;210:901-8
[xxi] Schulz R, Beach SR. Caregiving as a Risk Factor for Mortality. : The Caregiver Health Effects Study. JAMA Dec 15 1999;282(23):2215-19
[xxii] Emanuel E, Emanuel LL. Four models of the physician –patient relationship. JAMA 1992;267(16)2221-6
[xxiii] Buchsbaum DG, Buchanan RG, Welsh J et al. Screening for drinking disorders in the elderly using the CAGE questionnaire. J Am Geriatr Soc 1992;40(7):662-5
[xxiv] Parmelee, Patricia A.; Katz, Ira R. Geriatric Depression Scale. Journal of the American Geriatrics Society, Vol 38(12), Dec 1990, 1379.
[xxv] Scandrett KG, Zuckerbraun BS, Peitzman AB. Opertaive risk sttrification in the older adult. Surg Cli N Am 95(2015) 149-72
[xxvi] Partridge ISL, Harari D, Martin C, Dhesi JK. The impact of preoperative comprehensive geriatric assessment on postoperative outcomes in older patients undergoing scheduled surgery: a systematic review. Anesthesia 2014;69 (Suppl.1)8-16
Users are free to download and distribute Geriatric Fast Facts for informational, educational and research purposes only. See Term of Use for additional information.
Disclaimer: Geriatric Fast Facts are for informational, educational and research purposes only. Geriatric Fast Facts are not, nor are they intended to be, medical advice. Health care providers should exercise their own independent clinical judgment when diagnosing and treating patients. Some Geriatric Fast Facts cite the use of a product in a dosage, for an indication, or in a manner other than that recommended in the product labeling. Accordingly, the official prescribing information should be consulted before any such product is used.